Thiel-Linked HHS Nominee Threatens MAHA Ambitions with Biotech Stance
Late last November, President Donald Trump announced Jim O’Neill as his nominee for deputy secretary of Health and Human Services (HHS), where he would work under Robert F. Kennedy Jr., Trump’s pick for HHS secretary upon confirmation. As deputy secretary, O’Neill would essentially function as the Chief Operating Officer of the department, overseeing “the day-to-day operations of all sub-agencies” as well as leading “public health emergency preparedness,” i.e. the government’s policy responses to bio-terror events, pandemics, etc. In addition, O’Neill would “oversee the development and clearance of HHS regulations” and ostensibly be the main implementer of the “Make America Healthy Again” (MAHA) policy agenda.
Built on a promise to eliminate industry capture of public health regulatory agencies and curb the influence of Big Pharma and Big Food, Robert F. Kennedy Jr.’s MAHA movement played a crucial role in funneling would-be Kennedy voters into the Trump camp. MAHA, in essence, granted the Trump campaign a tinge of populist legitimacy among Covid era dissidents, which grew out of the shuttering of RFK Jr.’s independent presidential run.
However, O’Neill’s business connections, both past and present, as well as his previous statements on public health policy, strongly suggest that he is not only unlikely to implement the policies that MAHA-centric voters are expecting, but that he may in fact pursue an agenda that stands in direct conflict with the main tenets of the MAHA movement. Specifically, he advocates reforming the FDA to deregulate and accelerate the pathway from drug development to legalization. This would notably aid the biotech industry, which has long struggled to get its products approved outside of an “emergency”-based deregulatory paradigm.
When considering the investments and board positions that O’Neill himself has made and held in biotechnology companies, this would likely include mRNA products that Kennedy and other MAHA influencers have spent years criticizing since the Covid-19 pandemic — a clear contradiction between O’Neill’s views on public health, and those which the MAGA base were sold on the campaign trail.
Perhaps standing in even starker contrast with MAHA principles, O’Neill currently sits on the board of a company that is currently pursuing the development of a neurotoxic substance as a “therapeutic” treatment for people with Alzheimer’s disease (a neurodegenerative disease). Ironically, that same substance has long been flagged by Kennedy and the organization he co-founded, Children’s Health Defense, as one of the main causative agents in their hypothesis for a vaccine-autism link and other chronic conditions suffered by many Americans, particularly children.
In addition to O’Neill’s biotech connections, he also boasts significant ties to the CIA-linked company Palantir and its co-founder Peter Thiel. Palantir, notably, is undertaking considerate efforts to apply a pre-crime paradigm to public health events, mainly through its several significant contracts with HHS that would greatly determine the nature of the “public health emergency preparedness” that O’Neill will directly oversee. Several of these contracts date back to the first Trump administration, when Palantir played a major role in the military-run Covid-19 biosurveillance and vaccine development / distribution program known as Operation Warp Speed – a program that has been heavily criticized by both Kennedy and the broader MAHA movement.
Indeed, Palantir has since further entrenched its role within the HHS apparatus, most recently via the CDC’s Center for Forecasting and Outbreak Analytics (CFA), a disease forecasting and mass biosurveillance program that Palantir runs significant amounts of data for.
Also indirectly connected to this CDC effort is Bill Gates, as the former vice-president of the Gates-connected Cascade Investment firm, Dylan George, now runs the CFA. Importantly, the Gates Foundation has significant investments in biotechnology, an industry that notoriously faces strenuous regulatory difficulties in getting its products through the standard Food and Drug Administration (FDA) approval process. As a result, prominent players in the biotech industry, including Gates as well as others like Trump surrogate Vivek Ramaswamy, have embarked on an effort to dismantle the current regulatory paradigm and replace it with one friendly to “innovation,” or in other words, one with significantly less rigorous standards.

Unlimited Hangout previously reported on the industry players tackling this problem on the global scale, and it seems that now, with O’Neill poised to be at the helm of “development and clearance of HHS regulations,” experimental biotech may finally gain the unfettered access to the American market it needs.
As this article will demonstrate, O’Neill himself also stands to benefit financially if his desired regulatory model is achieved, as do key members of Trump’s cabinet. Further, given the pandemic preparedness model of monitoring and developing preemptive countermeasures for pathogens with pandemic potential, as well as the Big Tech surveillance that coincided with the distribution of the experimental Covid-19 vaccines, it appears likely that biosurveillance will play a crucial role in the future of the biotech market — especially a deregulated one. Such a model would notably benefit the public-private surveillance infrastructure built up by the man who helped kickstart O’Neill’s private sector career, Peter Thiel.
Yet, O’Neill’s role in the now-decades long effort to provide accelerated, deregulated paths to market for experimental drugs dates back to his time in public office, where he served during the height of the now infamous War on Terror. It was likely there that he first met George W. Bush’s HHS Secretary, Tommy Thompson, who implemented the consequential Project Bioshield Act of 2004 — a piece of legislation that marked a firm step forward in the path towards “emergency” deregulation of drugs and vaccines.
O’Neill’s Early Forays in Public Health: From Bird Flu Panic to Project BioShield
After attending elite universities like Yale University and the University of Chicago, Jim O’Neill landed a job in the George W. Bush administration, first at the Department of Education and then at HHS. He began his new role at the end of 2002 as director of the Speech and Editorial Division, where he led the speechwriting team for then-HHS Secretary Tommy Thompson and did the same for the first several months of the tenure of Thompson’s successor, Mike Leavitt.
The latter years of O’Neill’s tenure in this position are particularly notable, as many of Thompson’s and Leavitt’s speeches between 2004 and 2005 focused on fearmongering over the threat of pandemic “bird flu,” specifically H5N1, which were later deemed overblown. Much of the fear propagated by Thompson and others during this time about bird flu were notably based on the doomsday predictions offered by the now heavily-discredited British epidemiologist Neil Ferguson of the Imperial College London. Several of Thompson’s speeches before Congress, which O’Neill presumably helped write, demanded significant funding for flu vaccine stockpiles and to help vaccines switch from traditional vaccine production methods to “a new cell-based technology.” Upon his resignation in December 2004, Thompson stated that his greatest concern at that time was bird flu, which he referred to as “a really huge bomb […] that could adversely impact on the health care of the world.” Leavitt was even more effective than his predecessor at causing fear in the public and thereby generating public support for ultimately unnecessary flu vaccine and antiviral stockpiles. According to O’Neill’s LinkedIn profile, several of the “major policy addresses” he developed for both Thompson and Leavitt dealt specifically with “pandemic influenza.”

Even though the fearmongering of Thompson and Leavitt along with other “experts” was unwarranted, the panic their speeches and public comments generated ensured that the U.S. government spent over $7 billion on combating the bird flu “threat” by purchasing significant quantities of medications like Tamiflu, an anti-viral produced by Gilead. Notably, Gilead’s former chairman was then-Secretary of Defense Donald Rumsfeld. Gilead’s stock price had dipped in 2003 before the bird flu concerns emerged, and when panic around bird flu arose the company saw its revenues quadruple. Rumsfeld sold some of his Gilead shares when the fearmongering began, and he was estimated to have netted at least $5 million. At the end of 2004, his financial disclosure report revealed that he still held $25 million in Gilead stock.
Many of those pre-emptive Tamiflu purchases for this “emergency stockpile” that were never ultimately needed (and justified using faulty modeling) were made through the Biomedical Advanced Research and Development Authority (BARDA). BARDA was established by the 2004 Project BioShield Act, which Thompson and his speechwriters heavily advocated for. The Bush administration justified the passage of this legislation in part by citing the dangers of the 2001 Anthrax attacks (a US military-linked false-flag tied to many of the same people who ultimately helped create and profited from BioShield and BARDA). Some of those figures would also go on to lead the government response to Covid-19 under the first Trump administration.
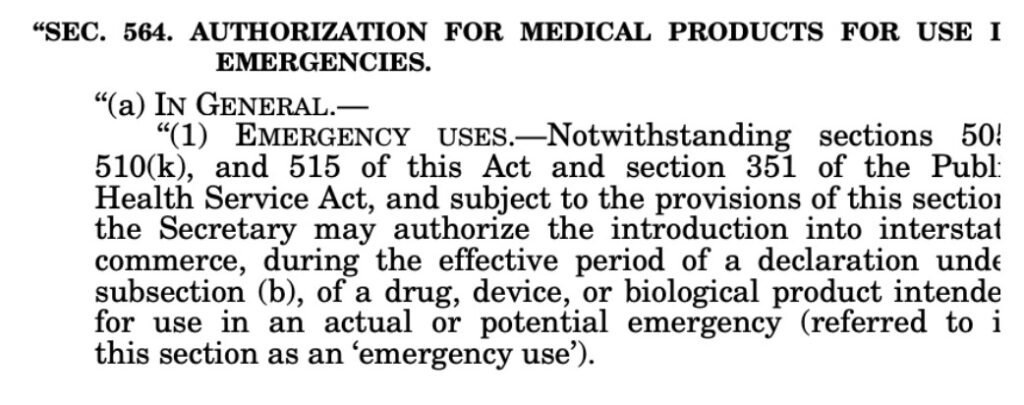
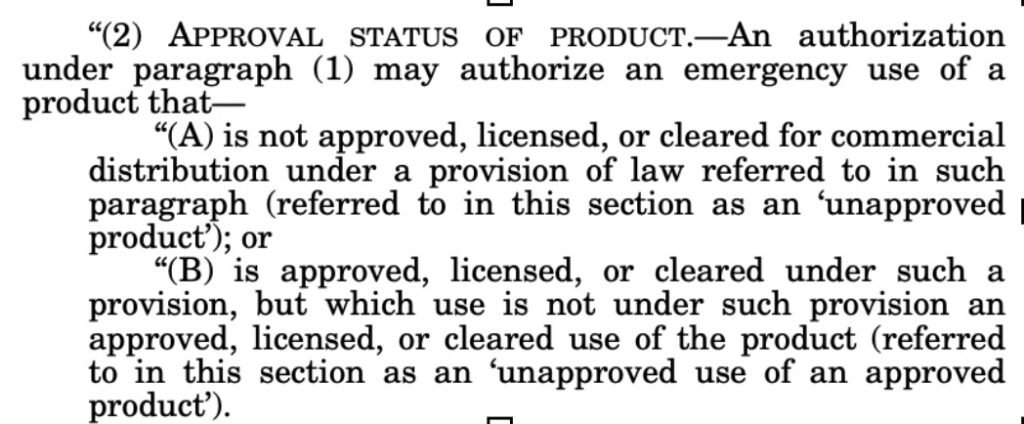
Beyond lining the pockets of Rumsfeld and Gilead through its mandate to create emergency drug stockpiles to thwart “bioterrorist” attacks, Project Bioshield also significantly advanced the emergency deregulation pathway for unapproved drugs—which notably saved Moderna from collapse during the Covid-19 pandemic 15 years later. Specifically, Project Bioshield granted the authorization of the “emergency use” of drugs that are “not approved, licensed, or cleared for commercial distribution” in the context of a potential or actual emergency.
Notably, O’Neill – after helping to write speeches that helped justify the creation of BARDA and the stockpiling of Tamiflu – joined the BARDA steering committee in 2006 and served in that capacity through 2008, the timeframe when many of these questionable Tamiflu purchases were actually made. A few months before joining BARDA’s steering committee, O’Neill had been promoted to the post of Associate Deputy Secretary and senior advisor to the Deputy Secretary in August 2005. During that time he oversaw policy for the CDC and worked on “emergency preparedness” and “homeland security.”
Presumably due to his utility to Thompson and his successor Mike Leavitt, O’Neill was again promoted, this time to the post of Principal associate deputy secretary of HHS in 2007, holding that position for close to a year. Again, O’Neill played an important role in developing pandemic preparedness policy and also focused on advising the HHS secretary and deputy secretary on homeland security, and in that capacity “led special projects related to policy and operations.”
After leaving the Bush administration, O’Neill became involved with Peter Thiel, who had previously helped the architects of mass surveillance during the Bush administration privatize its most controversial program, resulting in what is now the company Palantir. O’Neill began working as managing director at Thiel’s now-defunct Clarium Capital, a macro hedge fund that Thiel created shortly after selling PayPal to Pierre Omidyar’s eBay in 2002. O’Neill, relatively shortly thereafter, became head of the Thiel Foundation in 2009. There, he worked with Peter Thiel to create the foundation’s Thiel fellowship, which helped kickstart the careers of now prominent figures in military contracting (e.g. Palmer Luckey of Anduril), cryptocurrency and finance (e.g. Vitalik Buterin of Ethereum) and longevity-focused biotech (e.g. Laura Deming).

Around this same time, O’Neill became involved with the longevity-focused SENS research foundation, joining its board of directors in 2010 – a post he would hold through 2021. O’Neill also served as SENS’ CEO from 2019 to 2021, where he directed research focused on curing age-related diseases like Alzheimer’s. As will be noted again later, SENS’ earliest and most significant donor was Peter Thiel.
As Clarium Capital’s fortunes waned in the aftermath of the 2008 economic crisis, Thiel teamed up with Ajay Royan to create Mithril Capital in 2012, with O’Neill serving as founding managing director. At this point, O’Neill left his post at the Thiel Foundation to work full-time at Mithril. While at Mithril, O’Neill oversaw current Vice President J.D. Vance, who joined Mithril in 2016 as a junior investor and left the firm in 2018. While at Mithril, O’Neill handled significant investments in some notable biotech companies as well as investments in the Thiel co-founded Palantir, which – as previously mentioned – controversially contracts with HHS and important HHS sub-agencies with major implications for public health, privacy and future pandemic response. O’Neill left Mithril in 2019, the same year that the firm came under FBI investigation for financial misconduct (those allegations, however, focused largely on firm co-founder Ajay Royan). 2019 was also notably the year that one of the companies Mithril had backed, uBiome, also came under FBI scrutiny, later resulting in its founders being charged with health care fraud conspiracies.
O’Neill’s Connections to the Biotech Industry
During O’Neill’s tenure in a top position at Mithril, the venture capital firm invested in several significant biotech companies. These include uBiome, which was also backed by Andreessen Horowitz and the Sam Altman-run Y-Combinator. The company was founded in 2012 “to sequence the microbiome,” allowing patients to “explore their microbiome” via the company’s microbial genomic test and their possession of the “largest microbiome database in the world.” The company’s series B funding was led by 8VC, the venture capital firm created by Palantir co-founder and Thiel associate Joe Lonsdale. The company was later caught overbilling patients, pressuring them to take multiple tests when it was unnecessary, and also pressuring doctors to approve tests, including for patients with no symptoms. The FBI raided the company’s offices in 2019. In 2021, the co-founders were each charged with more than 40 criminal counts, including healthcare, securities and wire fraud.
Another biotech company backed heavily by Mithril during O’Neill’s time as managing director is Fractyl Health, which Mithril began funding in 2014. Fractyl has been developing 2 products, Revita – an outpatient procedure that modifies the lining of the colon to target obesity and type 2 diabates, and Rejuva – a “one-time gene therapy” targeting the pancreas meant to “enable durable weight loss and long-term remission of type 2 diabetes.” Neither of the company’s products have been approved by the FDA and clinical studies on them have yet to be performed, despite the company having been in business for over a decade — representative of a common trend in biotech companies struggling to get drugs through clinical trials.
The chair of Fractyl’s board is the co-founder of Mithril alongside Thiel, Ajay Royan. Another board member, Marc Elia, sits on the board of the Mithril-backed biotech firm Invivyd (formerly Adagio Therapeutics). Also on the board of Fractyl is former U.S. Senator Bill Bradley, who is also on the board of the Mithril-backed fintech and stablecoin-issuing firm Paxos. Bradley’s connections in tech also extend to figures adjacent to Jeffrey Epstein, as Bradley was notably affiliated with Ghislaine Maxwell’s husband Scott Borgerson and his firm Cargometrics—a satellite surveillance company that offers “unique data products and [software] solutions broadly to the investment management and maritime shipping & logistics markets.”
O’Neill has also had several notable connections to other biotech firms following his departure from Mithril in 2019. These include Oisin Biotechnologies, where O’Neill was a board observer from 2019 to 2021. Oisin develops therapies focused on longevity and “age-related diseases” that leverage a “new-non-viral delivery technology” they call Fusogenix Proteo-Lipid Vehicle.
That platform “enables extensive extrahepatic biodistribution for both DNA and RNA payloads.” The Fusogenix platform was not developed by Oisin directly, but by their partner firm Entos, which used the same platform to develop a “Covid-19 plasmid DNA vaccine” as well as several genetic treatments targeting obesity. Entos has four partner organizations/companies — three of them are Eli Lilly, the Bill & Melinda Gates Foundation and Oisin. John Lewis, the founder and CEO of Entos, co-founded Oisin in 2016 and has long served (and currently serves) as the Chief Science Officer of the company, further revealing the close association between the two companies.
O’Neill became involved with Oisin through his leadership roles at the SENS Research Foundation. During O’Neill’s time on the foundation’s board, SENS granted Oisin with an unlisted amount of seed-funding from SENS.
Notably, during his time at SENS, O’Neill served on the SENS board with a few important Thiel-associated figures. These include Blake Masters – a close Thiel associate who co-wrote a book with Thiel, served as COO of Thiel Capital and as head of the Thiel Foundation – as well as Kevin Dewalt. Dewalt maintained a position as the director of Strategic Alliances for the CIA’s venture capital arm In-Q-Tel from 2005 to 2008. During that same period, Dewalt also worked with the Thiel-founded Palantir – specifically Palantir’s Stephen Cohen – to “deploy the company’s first AI product in the US Intelligence community.” Palantir’s earliest funder, aside from Thiel himself, was In-Q-Tel.
Some of those involved in “longevity” research importantly believe that AI and other emerging technologies will play a significant role in developing life-prolonging-tech. The SENS Research Foundation focuses on longevity research and many of its members, including its founder, believe that medical technology is capable of granting near-immortality to humans, if not immortality itself. The foundation’s first major donor was Peter Thiel, who has injected millions into the foundation since its inception.
According to his LinkedIn, O’Neill has only served on the board of directors of one biotechnology company, ADvantage Therapeutics, which he joined in March 2023. He continues to serve on the board, but will ostensibly recuse himself from that role if confirmed as HHS deputy secretary. ADvantage does not reveal its board of directors on its website, and thus O’Neill’s involvement is not visible there, but his position on the company’s board is noted in their SEC filings.
ADvantage as a company focuses on neurogenerative diseases, specifically Alzheimer’s. Their main product is a compound called AD04, previously known as Alhydrogel. It is an aluminum-based vaccine adjuvant (aluminum hydroxide) that has been used historically in human and animal vaccines, but ADvantage Therapeutics seeks to transform this adjuvant into a “therapeutic” for Alzheimer’s patients.
The origins of ADvantage as a company, and the quest to turn AD04 into an Alzheimer’s treatment, date back to a study that tested a failed Alzheimer’s vaccine candidate called AD02, produced by the Austrian company AFFiRiS. In the Phase 2 clinical trial of AD02, the group that received the vaccine fared significantly worse than the control group. Both the control group and the group that received the AD02 vaccine received doses of the vaccine adjuvant AD04.
Instead of considering that the AD02 vaccine significantly worsened the outcomes of Alzheimer’s patients, they instead concluded that the aluminum-based compound AD04 had actually made patient outcomes significantly better. This is despite the fact that aluminum toxicity has been studied as a factor in causing Alzheimer’s disease, as aluminum is a known neurotoxin. In addition, independent scientists outside the company did not share the conclusions of the AFFiRiS scientists. While company scientists claimed that the control group data showed “evidence of disease modification”, other unaffiliated scientists argued that the data implied no effect at all, as the correlations observed in the control group are also known to “occur in the absence of treatment.”
Despite the lack of data or consensus suggesting that injecting Alzheimer’s patients with a known neurotoxin would lead to better patient outcomes, the AFFiRiS scientists doubled down and acquired the patent rights to AD04. They then teamed up with Agustin Fernandez, a Cuban-born movie producer, and his business partner Jeffrey B. Madden to create ADvantage Therapeutics to commercialize AD04 as a treatment for Alzheimer’s. Notably, the ADvantage website notes that the initial AD02-AD04 study did not contain data supporting the use of AD04 as a “therapeutic entity”, and that the company and its founders are unable to explain how AD04 allegedly functions to reduce Alzheimer’s pathology.

Despite this admitted lack of evidence, the company is conducting pre-clinical trials in parallel to the clinical development of their AD04-based therapeutic as an attempt to shore up data that shows the compound has therapeutic potential. However, elsewhere on its website it treats AD04 as having passed Phase 2 clinical trials (and entering Phase 2b), but this seems to be a misleading reference to the original AFFiRiS study, characterizing it as a study that was testing for the effects of AD04. In reality, the AFFiRiS study was a Phase 2 trial for the failed AD02 vaccine, and was not a trial meant to test AD04.
In addition to AD04, the company is also attempting to develop two other products, AD09 and AD15. AD09 has an undisclosed mode of action, but appears to be a mRNA product based on the information provided on the company’s website. AD15 is also a mRNA product based on the Klotho protein, which can reduce symptoms of aging when over-expressed. The scientist who discovered the Klotho gene, Dr. Makoto Kuro-o, joined ADvantage as a member of its scientific advisory board in early 2024. As of late last year, the development of AD15 was spun-off from ADvantage Therapeutics and into a different company called Klothea.
According to a company press release, O’Neill’s appointment to the board of directors was aimed at facilitating the approval of AD04, the aluminum vaccine adjuvant, as well as its mRNA products. In the press release, CEO Jeffrey Madden was quoted as saying “The addition of Jim to our Board of Directors signals the next level of development for our company […] As we embark upon our confirmatory Phase 2b study for AD04 in early Alzheimer’s disease, we are fortunate to have Jim’s talents and experience to guide us during this exciting time.” Madden also stated that “Jim’s deep expertise in longevity will serve us well as we develop our mRNA technology to fight pathologies of aging by advancing and sustaining the capabilities of klotho, which many consider the longevity gene. We are developing platform technology to create a pipeline of [targets] to tackle the most common diseases of aging by using the klotho protein. We look forward to Jim’s guidance in this area.”
O’Neill himself had high praise for the company’s AD04 product, stating that “AD04 has the potential to radically improve the lives of millions. I am excited to collaborate with ADvantage to help propel it forward.” Even if he does recuse himself from ADvantage’s board of directors upon confirmation, his top role at HHS – where he will oversee the removal and creation of regulations at the FDA and other HHS agencies – would certainly place O’Neill in a position where he could propel products like AD04 forward.
O’Neill’s enthusiasm for turning an aluminum adjuvant into a therapeutic for a neurodegenerative disease clashes directly with past statements from incoming HHS Secretary Robert F. Kennedy Jr. For example, in his book Vax-Unvax: Let the Science Speak, co-written with Dr. Brian Hooker, Kennedy characterizes aluminum adjuvants as harmful to human health and as one of his major concerns with respect to vaccine safety. In addition, the Kennedy-affiliated organization Children’s Health Defense, in addition to publishing the aforementioned book by Kennedy and Hooker, has published many articles over the years warning of the dangers of aluminum vaccine adjuvants and have directly linked vaccines containing aluminum with adverse vaccine side effects, especially in children, as well as the increasing incidence in childhood autism rates. Unlimited Hangout reached out to Children’s Health Defense for comment on aluminum vaccine adjuvants and the attempt to commercialize one of them as a therapeutic, but did not receive a response prior to publication.
O’Neill’s significant biotech connections do not end there. He served as a “global health adviser” to Rational Vaccines, a company that, based on its founders and board, is deeply connected to ADvantage Therapeutics. The co-founders of ADvantage, former film producer Agustin Fernandez and CEO of ADvantage Jeffrey Madden, also occupy important roles at Rational Vaccines. Fernandez was the co-founder and is the current CEO of the company, while Madden sits on its board and is a lead investor.

The company is focused on treating herpes, mainly through the creation of a herpes vaccine. It was awarded $2.8 million by the National Institute of Health (NIH) to further its herpes product development, including a test that enables “routine population-based screening” of Herpes Simplex Virus (HSV) with higher sensitivity than other tests, and a vaccine to curb the spread of herpes—which the company calls a “global pandemic.”
The company’s focus on herpes, however, has not stopped it from developing biotechnology for Covid-19. It is currently developing a “serological assay” Covid-19 test, which the company claims boasts higher sensitivity compared to currently available tests. This is apparently due to its ability to test for “antibodies to most viral proteins,” as opposed to a “single or small subset of viral proteins.” Rational Vaccines developed the blood assay technology by repurposing its herpes tests, and is notably employing the same technology behind their herpes vaccine candidate to develop a Covid-19 vaccine. According to the company, they are “in the process of adapting [their] HSV immunotherapeutic candidate, RVx201, to a viral vector format” in order to “enable the development of multiple vaccine types, including to SARS-COV-2.”
While Rational touts its ability to repurpose its herpes vaccine technology for other immunizations, the company’s long and sordid history of unethical regulatory obfuscation paints an unsettling picture of any future product it develops.
The questionable nature behind Rational Vaccines’ business practices began before the company’s inception. In 2013, the co-founder of the company, the late Southern Illinois University professor William Halford, administered doses of a shot that contained a virus he had created “at a Holiday Inn Express and a Crowne Plaza Hotel that were a 15-minute drive from [his] SIU lab.”
Halford’s unconventional methods continued in the years to come, and importantly at Rational Vaccines itself. After he co-founded Rational Vaccines with Fernandez, he ran an offshore clinical trial from a house in the Caribbean Islands for the company’s herpes vaccine. Halford utilized American participants, most of whom Rational Vaccines claims were “Americans with herpes who were flown to the island several times to be vaccinated,” as reported by Kaiser Health News. However, the trials were entirely unmonitored — neither by the FDA or any institutional review board.
Robert Califf, Obama’s former FDA commissioner, told Kaiser Health News that “he couldn’t think of a prior instance in which American researchers did not set up an IRB abroad.” Califf did note, however, that doing so “may be legal.”
On a side note, Califf’s critiques of Halford’s trials appear odd, given Califf has spent much of his career dedicated to implementing the principles of the Fourth Industrial Revolution into public health. Among these principles involve a deregulated drug development process that replaces the standard randomized clinical trial with a technocratic, “innovative” approach. While Califf headed the Duke Clinical Research Institute, the institute co-founded an initiative which aimed to create more “efficient clinical trials,” namely by “maximally [leveraging] available clinical and nonclinical data, including data collected via digital technologies, to minimize collection of necessary trial specific data,” or in other words, prioritizing the use of medical data collected outside of a clinical trial setting. Instead, the prioritized data in this model would be extracted from novel sources (such as digital technologies like wearables) and be “interoperable,” maximizing the capacity for “all researchers and sponsors” to see and share that data.
Despite experts slamming the experiment as unethical, Fernandez claimed that he knew of “individuals who experienced positive outcomes from the vaccine,” effectively downplaying the dangerous methodology used during the testing.
One of Rational’s most prominent early donors, former managing director of Credit Suisse Bartley J. Madden, was intrigued by Halford after hearing him talk about his work at a symposium at Southern Illinois University. According to Wired, Madden “wrote a book called Free to Choose Medicine, which argues that the FDA’s risk-averse approach to drug approval gets in the way of innovation and keeps life-saving medicines off the market.”
As he describes in his book, A Foundational Explanation of Human Behavior, “The conventional goal of safe and effective drugs leads to a relentless demand for ever more expensive clinical testing demands, sky high prescription drug prices, and, importantly, delayed access to life-changing medical treatments. I argue that the appropriate goal is better drugs, sooner, at lower cost. The key constraint is the hugely expensive (time and money) FDA clinical testing process.” Fittingly, in Bart Madden’s eyes, “Halford embodied the part of the brilliant outsider tangling with the scientific establishment.” While Madden claims that he wasn’t aware of the offshore trials at the time of his donation, his own beliefs on regulation appear in line with Halford’s methods.
Also notable is that Jeffrey B. Madden—CEO of ADvantage Therapeutics and prominent investor in Rational Vaccines — is a board member and the Treasurer of Bartley J. Madden’s Bartley J. Madden Foundation. Bart Madden previously worked in the US Army where he was “involved with classified weapons development/testing” before his private sector finance career took off. While a familial connection between the two does not appear to have been established, the work of both has obviously intersected greatly through the world of biotech, an industry that would benefit significantly from Bart Madden’s deregulated vision of drug development.
Likewise, the regulatory evasion and safety controversy did not stop O’Neill’s associate Peter Thiel from investing $4 million in the research, with the caveat that future testing comply with FDA standards. While Thiel’s caveat indicates disapproval of Halford’s brazenly dangerous methods, Thiel does believe regulations stand in the way of progress. As the Kaiser Health News story notes, Thiel previously said that the FDA’s standards are so cumbersome that “you would not be able to invent the polio vaccine today.”
Eliminating Efficacy Testing in the Name of “Innovation”
O’Neill himself has long echoed the deregulatory rhetoric of Peter Thiel, Bart Madden, Califf and others. In fact, O’Neill’s past statements on regulations may be even more blatantly controversial than his contemporaries — seeking to eliminate efficacy trials altogether. He previously made these opinions clear at the Hyatt Regency in Santa Ana, California during a 2014 talk for the SENS Research Foundation:
“We should reform [the] FDA so that it’s approving drugs after their sponsors have demonstrated safety and let people start using them at their own risk, but not much risk of safety…But let’s prove efficacy after they’ve been legalized.”
This speech first came under public scrutiny after it was reported in December 2016 that the first Trump administration’s transition team (of which Thiel was also a part) was considering O’Neill to head the FDA. O’Neill, at the time, was apparently deemed too controversial for the role and Scott Gottlieb was chosen instead. Gottlieb joined the boards of Pfizer and the CIA-linked biomanufacturing company Resilience shortly after his stint at the FDA concluded.
Notably, the current nominee to head the FDA, Johns Hopkins’ Martin Makary, has been deemed very friendly to the biotech industry. While Makary was a critic of Covid-19 lockdowns and some other policies, like vaccine mandates, he supported universal masking and early doses of mRNA Covid-19 vaccines. He also criticized the FDA during Covid-19 for being too slow to approve the “lifesaving” mRNA Moderna and Pfizer vaccines, arguing in a 2020 interview that the experimental vaccines should have been approved after Pfizer and Moderna’s application submissions within 24 hours. Mocking the FDA’s apparent dawdling on its review process, Makary called it “Operation Turtle Speed.” Upon his appointment to head the FDA for Trump’s second term, biotech industry leaders told STAT News they felt relief at Markary’s appointment, with one remarking we “dodged a bullet.” Other industry experts quoted by CNBC shared similar sentiments, with one stating that “we expect [Makary] will promote technology/innovation in a way that offers some reprieve for those that [are] fearing a department more aligned with different virtues.” In other words, it seems that Makary and O’Neill are quite aligned on deregulating the FDA drug/vaccine approval process.
O’Neill’s comments on the FDA, which he will oversee and greatly influence, ultimately fit into his larger plan to “[streamline] licensing and drug development and reducing time and costs” — which he remarked “was a big interest” of his during his time at HHS. Given his proximity to the centers of power that played an integral role in passing the consequential Project Bioshield Act of 2004, which authorized emergency use of unapproved medical products, this interest comes as no surprise. Notably, however, O’Neill’s advocacy in this context did not emerge from concerns of pandemic response or emergency situations, but instead from the desire to make biotechnology more viable, safe and attractive to investors.
This interest in “streamlining” drug development led him, per his own account, to “shut down” an effort by the FDA to start regulating In Vitro Diagnostic Multivariate Index Assays (IVDMIA), a kind of biotechnology used to diagnose “disease or other conditions,” or used to “cure, [mitigate, treat or prevent]” a disease. O’Neill used this story to segue into his controversial proposal to eliminate efficacy tests of drugs entirely, which he calls “progressive approval.” His calls for deregulation were met with applause from the crowd of academics, businessmen and investors present at the event.
O’Neill then proceeded to heap praise on the work of Richard Barker, founding director of Oxford’s Centre for the Advancement of Sustainable Medical Innovation, specifically his model of “adaptive licensing.” In essence, Barker’s model stands in direct conflict with the main principles of RFK Jr.’s MAHA agenda. While MAHA seeks to separate industry from public health agencies, Barker’s work focuses on infusing Big Pharma into the drug development process even further. He proposes this as a solution to what he describes as a problem so severe that it makes the current drug development process “not sustainable” — specifically, the alleged issue of those handling clinical development being “completely isolated” from those handling the commercial side of the process. He remarks that they remain “in their respective silos and report into different echelons of senior management,” and that as a consequence, “there is often a major disconnect between the clinical development program and the collection of value data.”
Barker’s solution is one eerily similar to Robert Califf’s aforementioned Fourth Industrial Revolution-inspired program at Duke. Barker believes that the utilization and collection of a massive array of “real-world data,” or data accumulated outside of clinical trial settings via unconventional sources, will solve this allegedly catastrophic problem. As Maddie Bannon described in her article on Robert Califf, real-world data “is collected from a vast array of sources including electronic health records (EHRs) submitted by medical professionals during a doctor or hospital visit, insurance claims and billing data, medical product and disease registries, the patient themselves (e.g. data submitted through an app), wearable devices, cellphones, and social media.”
This data, Barker says, can address the division between the commercial and scientific sides of development by integrating “value in the design of the clinical development, with an early crafting phase involving the input of regulators, payers, and patient associations, so as to ensure the collection of both clinical and value data.”
Further, he boasts that it can jack up drug prices by utilizing real-world data based on the surveillance of patients “to help establish the value of the product.” This would allegedly solve the problem of drug makers setting “the price as high as possible at the beginning of the process,” by allowing companies to continuously increase the price of a drug as they monitor its effects in the real world, using “compelling real-world data” as their justification for price hikes. In other words, Barker claims that a system should be in place to funnel mined biodata directly to drug manufacturers in order to alter the value of the product throughout its time on the market. Quite literally, this idea would allow Big Pharma to directly exploit the fragmented, data-mined parts of their customers to cultivate significant value and capital—a seemingly techno-feudalistic iteration of healthcare.
Yet this is not the only end Barker seeks to employ this data towards. In addition, he believes that mass profiling of patients should be used in order to “segment” communities “on a continuous basis” based on their medical needs. He claims that this would enable the industry to achieve its profits based on predicted, guaranteed “outcomes” as opposed to developing for volume. O’Neill recently expressed similar priorities on X (formerly Twitter) when he claimed that “Many Americans think we have free markets in health care. We don’t. Hundreds of bureaucratic rules, perverse incentives, and opaque pricing make health care more expensive and less efficient than it should be. Providers of care are usually paid by volume, not outcomes” (emphasis added).
This predictive, “outcome”-focused use of data would allow “products to be prescribed to and used by the right patient segment,” according to Barker. This line of thinking echoes the values of the mass surveillance based pre-crime, counterinsurgency culture that so many of the companies and figures surrounding Thiel pursue. It also bears striking similarities to Palantir’s Tiberius program that was used to distribute Covid-19 vaccines to AI-determined priority populations as part of Operation Warp Speed — which the CDC’s Center For Forecasting and Outbreak Analytics has since entrenched into HHS biosurveillance infrastructure.
However, Barker goes even further with this proposed strategy; he believes that when considering patients, “the industry needs to focus on the behavioral factors which drive adherence, either as accelerators or decelerators. The goal should be to collect evidence as to how to boost adherence, and the exercise is complex since there are many types of patients with different behavioral contexts and psychological barriers” (emphasis added). The breadth of data required to carry out such precise influence of behavior would obviously be vast, and comes out of a long term military strategy of weaponizing information.
This concept of utilizing knowledge accumulated from mass datasets to manipulate and direct human behavior dates back to J.C.R. Licklider’s time at the Advanced Research Projects Agency’s (ARPA) Behavioral Science and Command and Control division in the early 1960s, before the advent of modern computer networks. At least one of Licklider’s “Behavioral Science” schemes was performed under the auspices of standard military dealings, as his ARPA division deployed a project to study seemingly benign statistics of the Thai population “that sought to measure the body size of several thousand Thai military personnel to aid in the design of equipment and uniforms.” However, as Yasha Levine details in his book Surveillance Valley, beyond the physiological data the researchers collected, they also accumulated information on the participants’ ancestors, religion and their opinions on the king of Thailand. “The deeper purpose,” according to Levine, “was rooted in prediction and control.” Levine expounds on this idea by quoting Annie Jacobsen’s The Pentagon’s Brain: “If Thailand were to become a battle zone, ARPA would have information on Thai soldiers, each of whom could be tracked. Information — like who deserted the Thai army and became an enemy combatant— could be ascertained. Using computer models, ARPA could create algorithms describing human behavior in remote areas.”
Like Licklider’s strategy of utilizing data to control the “outcomes” of potentially insurgent populations in the Global South, Barker’s model relies on pushing populations towards the desired outcomes of bureaucrats that “trial participants” are likely unaware of. Both systems rely on the utility of seemingly neutral information to quell dissent, and ultimately manipulate (or even halt) what would be the organic decisions of people.
In addition, O’Neill’s views on ending efficacy testing would likely prove incredibly useful to the biotech industry, particularly those that manufacture mRNA products. Prior to the Covid-19 crisis, which facilitated emergency deregulation, mRNA products struggled to get to market under the existing regulatory paradigm. This is largely because most mRNA products struggle to be both safe and effective, as increasing effectiveness has tended to dramatically decrease safety while ensuring safety has tended to dramatically decrease efficacy. Thus, eliminating efficacy trials would allow mRNA products that have been unable to prove both safety and efficacy a much better chance at making it to market.
A telling example of this persistent issue in the mRNA industry is the company Moderna. Prior to its Covid-19 product, Moderna could not get a single mRNA product approved for over a decade and struggled to even get its products through animal testing. This issue for the company was largely based on its lipidnanoparticle (LNP) delivery system for mRNA. According to reporting from STAT News, this delivery system “created a daunting challenge [for Moderna]: Dose too little, and you don’t get enough enzyme to affect the disease; dose too much, and the drug is too toxic for patients.” Many major mRNA-focused companies, like Pfizer partner BioNTech and Vivek Ramaswamy’s Roivant, have bet heavily on this same LNP delivery system despite its dubious record, resulting in numerous legal snafus related to who exactly owns the rights to which aspects of that delivery system. It would be these types of companies that would stand to benefit the most from O’Neill’s prior proposals to eliminate efficacy testing for vaccines and other products, freeing them from long-standing concerns about their mRNA delivery mechanisms.

O’Neill’s Proximity to Palantir and What it Means for HHS’ Approach to AI
The merging of Big Tech, Big Healthcare and the public sector are part and parcel to the emergency deregulatory framework that O’Neill appears to support, both through his own statements and his business associations. It turns out that O’Neill has dabbled in all three of these ever-harder-to-distinguish sectors. As this article has previously noted, biosurveillance works in tandem with accelerated drug development, as the lack of regulatory scrutiny in these contexts provides the perfect pretext to justify the surveillance of those who receive the “experimental” drugs. This notably occurred during Operation Warp Speed. It just so happens that the government contractor on the front lines of this increasingly pervasive industry is Palantir, which was co-founded by O’Neill associate, Peter Thiel. Thiel remains the company’s leading investor. In addition, the VC firm of another Palantir co-founder, Joe Lonsdale, is deeply connected to the CIA-linked firm that produces the mRNA for Moderna’s Covid-19 vaccine, among others. Lonsdale has publicly praised O’Neill’s appointment as HHS deputy secretary, with O’Neill responding that Lonsdale has “greatly inspired me for a long time.”
While Palantir’s work with HHS dates back to at least 2010, the data company has become increasingly entrenched within HHS, influencing policy, resource allocation and more since the Covid-19 pandemic. Palantir gained major contracts with HHS during the Covid-19 era, particularly during the last year of the previous Trump administration. These included Palantir’s outbreak warning and wastewater surveillance system, HHS Protect, and its vaccine allocation program, Tiberius. The Covid-19 era FDA/Palantir program 21 FORWARD, which helped experts examine how Covid-19 incidence rates might affect the food supply, has expanded into a crucial part of the FDA’s “food supply chain disruption monitoring and crisis response.” The pre-crime operation turned predictive health iteration of DARPA, ARPA-H, tasked Palantir last year with running its core data infrastructure. Yet, arguably most importantly, in 2022, the two entities united a myriad of the Palantir and HHS/CDC biosurveillance programs together under the CDC’s “Common Operating Picture,” which aims to secure “strong collaboration across the federal government, jurisdictional health departments, private sector entities, and other key health partners.”

Preceding this pledge of CDC-Palantir unification was the announcement of the CDC’s Center for Forecasting and Outbreak Analytics (CFA) — a program dedicated to carrying out, among other things, the multi-sector goal of the CDC’s Common Operating Picture. Through a consortium of academic centers, private institutions and federal agencies all analyzing novel data sources, the CFA generates artificial intelligence (AI) forecasts of disease outbreaks in order to curate specified, targeted policy measures for specific communities/populations — purportedly to stop epidemics before they occur.
As Unlimited Hangout recently detailed, the policy implications for such a program could be vast. For example, the CFA’s data analysis and extraction will inform policies involving the “community migration” of individuals and/or populations; whether they are deemed “high risk” or not (with proceeding policy directly curated relative to a community’s/individual’s purported “risk level”); and key decisions on medical countermeasures during disease outbreaks. To demonstrate the “targeted” nature of the program, the CFA will likely factor in a myriad of “social determinants” in dictating such policy, including race, geography, household crowding and even financial data.

The material implications of CFA, therefore, stand to be huge — with Palantir guiding the ship, and Thiel’s associate Jim O’Neill overseeing it all. The conflicts of interest are apparent. O’Neill’s history of injecting funds into Palantir itself and Thiel-backed projects will likely not cease at HHS, and given Palantir’s full integration into the agency’s biosurveillance infrastructure, it may even expand. Such a possibility becomes even more likely considering one of the architects of the HHS Protect system that Palantir manages, Kristen Honey, was recently appointed HHS’ Chief Data Officer.
Further, beyond O’Neill’s connections to Thiel, his own positions on AI make him likely to uphold and support this predictive healthcare infrastructure. O’Neill has long been a vocal supporter of the “artificial intelligence-driven” healthcare system that CFA and Palantir are currently implementing, and which Big Tech, Big Healthcare and the Pentagon support. On X, O’Neill responded to a tweet from a biotech executive that called for the widespread use of “autonomous AI” to cut healthcare costs with a flowery endorsement: “AI is going to become essential across government and across health care….FDA and [Center for Medicare and Medicaid Services] can help doctors and patients by supporting rapid adoption.”
This proclivity for AI has seemingly characterized another new pick for Trump’s HHS. Meghan Dierks, the new HHS Chief Artificial Intelligence Officer, previously acted as “the chief data officer of San Francisco-based health care software company Komodo Health.” It was there that she “spearheaded the development and evaluation of AI-powered healthcare analytics tools for life sciences companies, healthcare practitioners, and patient advocacy groups.”
Interestingly, Komodo’s business model relies heavily on utilizing AI to tap and interpret “real-world data” in order to help pharmaceutical companies navigate the “uncharted waters” of commercial drug launches. This navigational data comes from the massive dataset the company has built “which ingests information from more than 15 million new patient encounters each day, capturing the anonymized experiences of more than 320 million Americans through disparate medical claims, diagnostic labs, and prescription data sets.”
This data comes to life through its Healthcare Map, which “follows the entire patient journey by utilizing analytics that go wider and deeper than any other data sources.” Almost as if the company emerged straight out of Barker’s “adaptive licensing” solutions, the breadth of data put to use via Komodo’s Healthcare Map “can discover patient populations that would benefit from their therapy; pinpoint patients that are not being treated at the standard of care; [and] identify medical centers most likely to recruit patients for clinical trials.” In other words, Komodo equips its clients to “segment” patients “on a continuous basis” based on their targeted medical needs — utilizing, sharing and likely expanding huge troves of data in the process.
However, Komodo’s mass AI data interpretation functions do not stop at drug launch assistance. Komodo can help with AI hospital management, as it enables “payors and employers [to] better understand referral patterns and patient flows, more effectively manage risk pools, and offer their members better care.” It also grants “local and national governments” predictive powers to “track outbreaks in real time, better estimate disease burden, and act more swiftly on behalf of the public.” The company’s entire model bears a striking similarity in function to the CDC’s Palantir-partnered CFA, which Unlimited Hangout recently reported on in great detail. Now, given Komodo’s connection to HHS via Dierks and its previous projects with the CDC, the tech company stands likely to be tapped by the CFA as a potential “data source” for the CFA’s many AI-healthcare goals.
In fact, this predictive infrastructure is deeply entrenched into other HHS / Palantir programs as well (beyond the CFA). For example, the Palantir-partnered ARPA-H — which was initially pitched to the Trump administration as a pre-crime program before its pivot into public health under Biden — recently selected and awarded four different “teams” to “develop bioelectronic devices to be implanted in patients through minor outpatient surgery.” While one team “aims to create a ‘Living Sentinel’ to measure key biomarkers in the body and monitor their condition in real-time,” all of the teams “aim to develop an implantable ‘Living Pharmacy’ programmed to deliver therapeutic molecules to the patient on demand for an extended period.” While ARPA-H pledges that the implantable chips will improve the care of people with a myriad of chronic conditions, this invasive technology also provides a new “novel” source of “real-world data” for Palantir to utilize.
The regulatory paradigm O’Neill seeks to implement will likely lead to huge gains for Thiel associates and Trump administration officials, ranging from Roivant co-founder Vivek Ramaswamy, to biotech investor JD Vance, to O’Neill, and Thiel themselves. Further, if efficacy trials are eliminated from the drug approval process, biosurveillance will likely be deemed the necessary alternative in order to “prove efficacy after [the drugs have] been legalized,” justifying the entire biosurveillance infrastructure built up by Palantir and its public sector partners.
Vaccine “Innovation” Seems Likely in New Trump Administration
Under O’Neill’s desired system, the entire biotech industry at large would be liberated from the regulatory hurdles that so often block its most “innovative” products from getting to market. Perhaps this is best demonstrated by prominent mRNA and biotech proponent Bill Gates’ recent praising of Trump. Gates, whom people often associate with the liberal side of the political spectrum, stated that he was “frankly impressed” with Trump after a “wide-ranging,” three hour discussion with the current President in which they discussed Gates’ ambitions for global health. They even both apparently got “pretty excited” when discussing the possibility of fast-tracking a HIV vaccine in the same manner that Trump enabled with the Covid-19 vaccine.

However, given Trump’s history with Gates during his previous term, Gates’ comments aren’t surprising. For instance, while Trump cut funding and left the World Health Organization in 2020, his administration continued to fund the Gates-backed GAVI vaccine alliance to the tune of a three-year pledge totaling $1.16 billion through the alleged CIA-front organization United States Agency for International Development (USAID). In April 2020, Trump lauded this partnership in a televised address to that year’s Global Vaccine Summit, stating “it’s great to be partnering with [Gavi]. We will work hard, we will work strong.” Notably, Gavi is one of the most prominent funders of the WHO, along with the Gates Foundation, and also co-led the WHO’s vaccine distribution program, COVAX, which “delivered nearly 2 billion doses of vaccines” across the globe. While Trump’s administration seemingly cut ties with the WHO during this period, it nevertheless supported at least one organization crucial to the WHO Covid response (i.e. Gavi).
In addition, the Trump administration itself arguably played a crucial in Gavi’s COVAX, as it funded, via Operation Warp Speed, some of the main vaccines that COVAX distributed. Gates personally yielded colossal returns on his investments in the Covid-19 vaccines, which were obviously aided by COVAX and the Trump administration’s fast-tracking of the vaccines themselves.
Gates’ recent comments, along with the ties of O’Neill and Vance to the biotech industry, suggests that the Trump administration will enable the proliferation of mRNA vaccine technology over the next four years. This notably indicates another betrayal of the MAHA movement, as the Trump-brokered era of Covid-19 “vaccine innovation” recently touted by Bill Gates has been long criticized by his incoming HHS Secretary Robert F. Kennedy. Indeed, in Kennedy’s book The Real Anthony Fauci, RFK demonstrated the integral role Gates played in Dr. Fauci’s “slow the spread, flatten the curve, wait for the jab” strategy of stopping the pandemic — specifically, in one instance, by literally orchestrating “homicidal” studies designed to kill clinical trial participants taking Hydroxychloroquine.
As Kennedy detailed:
“Dr. Fauci, Bill Gates, and WHO financed a cadre of research mercenaries to concoct a series of nearly twenty studies—all employing fraudulent protocols deliberately designed to discredit Hydroxychloroquine (HCQ) as unsafe…
Instead of using the standard treatment dose of 400mg/day, the 17 WHO studies administered a borderline lethal daily dose starting with 2,400mg on Day 1, and using 800mg/day thereafter. In a cynical, sinister, and literally homicidal crusade against HCQ, a team of BMGF operatives played a key role in devising and pushing through the exceptionally high dosing….
…Gate’s deadly deception allowed FDA to wrongly declare that HCQ would be ineffective at safe levels.”
Kennedy made these allegations as part of his larger argument that the medical establishment purposefully employed suspect and legally dubious methods to squander any chance that scientists might discover cheap, readily available medicines effective at treating Covid-19. This, he argued, allowed them to secure Emergency Use Authorization for the experimental vaccines. Based on this account, Gates played a crucial role in this grand scheme — committing medical “homicide” in the process.
RFK Jr.’s VP, Nicole Shanahan, said on the campaign trail that she and RFK were skeptical to endorse Trump because he had yet to acknowledge the failings of the vaccine-focused Operation Warp Speed. Now, Trump is negotiating with one of the most prominent perceived enemies of the MAHA movement, Bill Gates, to enact the exact same policy for at least one other vaccine.
To make things even more complicated for MAHA voters, Gates is not the only Big Tech executive seemingly giddy about the prospects of mRNA procurement under a Trump administration. Standing directly by Trump’s side at the White House to announce the $500 billion AI investment, Stargate, Oracle CEO Larry Ellison made utopian promises about the ability of rapidly produced and personalized mRNA vaccines to cure cancer, seemingly causing Moderna stocks to surge. These vaccines would be created via AI, according to Ellison — with data derived from AI-performed scans of patient blood being used to rapidly develop these personalized vaccines. Ellison’s comments, and the context of him making them at the announcement of a multi-corporation AI infrastructure program, suggest others in Silicon Valley and Big Healthcare are similarly excited for the prospects of “vaccine innovation” that appear poised to return in Trump’s second term.
Such a possibility is also supported by recent reports that Trump’s transition team sidelined two top Kennedy aides for their views on vaccines, with the Wall Street Journal writing that this development “underscor[es] a split over immunizations in the ‘Make America Healthy Again’ movement.” Citing Trump and Kennedy associates, the Journal stated that it seems more likely than not that the incoming administrations’ HHS policies “will have little do with vaccines.”
Further underscoring the subversion of Kennedy at HHS is the recent appointment of Heather Flick, a former senior official at HHS during Trump’s first term, to be Kennedy’s chief of staff. While at HHS, Flick began as the department’s general counsel and eventually worked her way up to become senior adviser to former HHS secretary Alex Azar. According to a former FDA official, Flick is acting as “sort of the Trump guys’ eyes and ears within the department, too; it’s a very important liaison and information source…The chief of staff, they kinda lay down the law.” Indeed, another former FDA official told Politico that the chief of staff’s role “can be very, very involved in FDA business and FDA work,” meaning Flick will presumably play an important role in drug regulation policy. For the MAHA movement, this is especially concerning given Flick’s important role at HHS at the same time that Azar declared Covid-19 an emergency and also contracted Palantir to run vaccine distribution and wastewater surveillance. This suggests Flick would be more friendly to the interests of O’Neill than Kennedy.

O’Neill’s appointment to be deputy secretary at HHS at the least undermines the promises that the Trump campaign made during election season to “Make America Healthy Again” voters. More likely, O’Neill’s position at HHS signifies the direction the Trump campaign will go in relation to public health — namely, that it will fully embrace the goals of the biosecurity apparatus that grew out of the post-9/11, pre-crime, neoconservative Total Information Awareness program that Palantir quietly shifted into the private sector. The biotech executives and investors surrounding Trump stand to reap huge profits from this agenda. In fact, they may need it to survive.
Touting RFK Jr.’s endorsement on the campaign trail may have subverted the chance for critical analysis of Trump’s policy positions (or lack thereof) on public health and pandemic preparedness. As a result, the MAHA movement presumably led many voters who were disaffected, betrayed and harmed by the policies of Operation Warp Speed back into the very hands of the man who touted and took credit for them them in the first place. With RFK Jr. acting as the public face of Trump’s HHS — all while the most powerful forces of the biosecurity agenda lurk in the shadows behind him — resistance to this agenda from within the administration appears doubtful despite the hopes of the MAHA voting bloc.
Thiel-Linked HHS Nominee Threatens MAHA Ambitions with Biotech Stance.